
CMS has announced a six-month nationwide moratorium on new Medicare enrollment for hospices and home health agencies.
Most headlines are focused on the freeze for new providers.
But existing hospice operators should pay attention to the larger message.
This is not just an enrollment issue. It is another signal that CMS is tightening program-integrity oversight across hospice.
According to CMS, the moratorium applies to new Medicare enrollment applications, including certain non-exempt changes in majority ownership. CMS also stated that the moratorium may be extended in six-month increments if the agency determines it is necessary. Existing enrolled providers are not automatically stopped from operating or billing because of the moratorium, but the policy direction is clear: hospice is under a much stronger program-integrity spotlight.
For existing hospice agencies, the takeaway is simple:
Documentation must be stronger before the chart is signed.
The Moratorium Reality: Existing Providers Are Still in the Spotlight
The moratorium does not stop existing Medicare-enrolled hospices from continuing to care for patients and bill Medicare when they remain compliant with Medicare requirements.
But it does confirm the direction of the environment.
CMS described the action as part of a broader effort to address fraud, waste, and abuse in hospice and home health. CMS also stated that it is using a data-driven approach, targeted investigations, and enforcement activity to identify and remove suspected bad actors.
That should matter to every hospice operator.
Not because every hospice is doing something wrong.
But because every hospice now needs to be prepared to defend the record.
In hospice, the risk is not only whether care was appropriate.
The risk is whether the documentation clearly supports the care, the level of service, the plan of care, and the patient’s continued eligibility.
Weak admission support.
Generic care plans.
Missing decline narratives.
Incomplete symptom follow-up.
Visit notes that do not clearly connect the patient’s condition to the hospice plan of care.
These are not minor documentation issues anymore. In the current environment, they can become survey findings, ADR exposure, payment risk, or audit risk.
Retrospective QA Is No Longer Enough
For years, many hospices have relied on a reactive QA model.
The clinician completes the visit.
The note is signed.
The QA team reviews the chart later.
Then someone has to chase down corrections, add clarifications, or identify gaps after the clinician has already moved on.
That model is becoming too slow for the current hospice environment.
Once a note is signed with weak eligibility support, missing follow-up, or a generic care plan, the risk is already inside the record.
The better model is proactive documentation defense.
That means surfacing documentation concerns while the clinician is still inside the workflow, before the note is finalized, and before the risk becomes harder to correct.
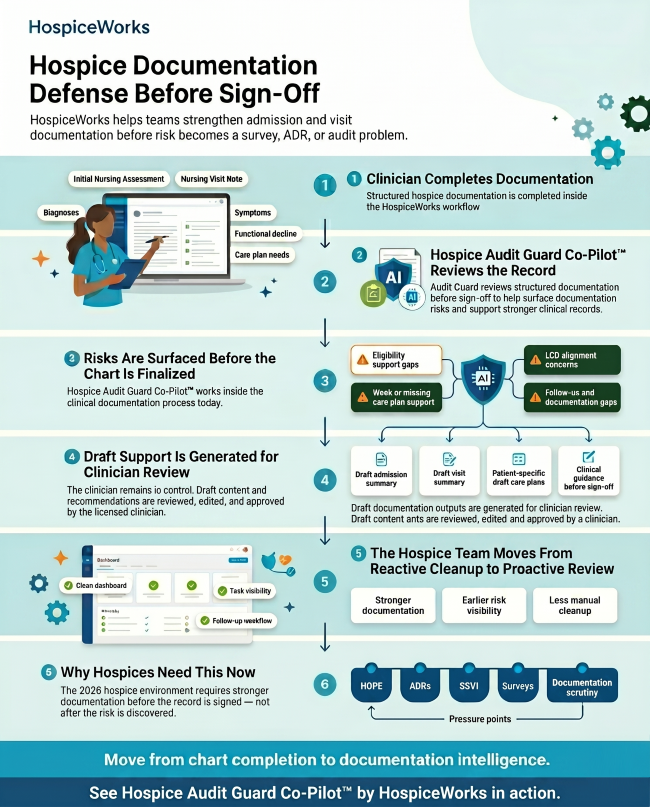
The 6-Step Defense: How Hospices Can Respond to Enhanced Oversight
The shift from reactive cleanup to proactive review is no longer optional.
Hospice teams need workflows that help strengthen documentation while the clinician is still completing the record.
- Clinician Completion Inside a Structured Workflow
Documentation defense starts at the point of care.
The clinician should complete the Initial Nursing Assessment, Nursing Visit Note, and related documentation inside a structured workflow that captures the clinical details needed to support hospice care.
That includes diagnoses, symptoms, functional decline, care plan needs, medication concerns, visit findings, and patient-specific changes.
A strong record does not happen by accident.
It happens when the EMR guides the clinician to capture the right information at the right time.
- Real-Time Review Before Sign-Off
Waiting until the end of the week to review documentation is too late.
Hospice teams need a process that reviews documentation before the record is finalized.
Hospice Audit Guard Co-Pilot™ by HospiceWorks reviews structured documentation before sign-off to help surface documentation risks, support stronger clinical records, and reduce manual cleanup.
The goal is not to replace the clinician.
The goal is to support the clinician while the record can still be strengthened.
- Risks Must Be Surfaced Before the Chart Is Finalized
The most important documentation issues should not be discovered days later.
They should be surfaced before sign-off.
Examples include:
Eligibility support gaps.
Weak or missing care plan support.
LCD alignment concerns.
Follow-up and documentation gaps.
When these issues are found early, the clinician can review the concern, add appropriate clarification, update the care plan, or strengthen the narrative while the patient encounter is still fresh.
That is a much stronger workflow than trying to repair documentation after the fact.
- Draft Support Should Be Generated for Clinician Review
Technology should support the clinician, not replace clinical judgment.
Hospice Audit Guard Co-Pilot™ by HospiceWorks can help generate draft admission summaries, draft visit summaries, patient-specific draft care plans, and clinical guidance before sign-off.
But the clinician remains in control.
Draft content and recommendations must be reviewed, edited, and approved by the licensed clinician.
This is the right balance.
The EMR helps reduce documentation burden and surface risk earlier.
The clinician makes the final decision.
- Hospice Teams Need to Move From Reactive Cleanup to Proactive Review
The old model creates too much cleanup.
The new model needs to create earlier visibility.
Hospice teams should be moving toward:
Stronger documentation.
Earlier risk visibility.
Less manual cleanup.
Cleaner dashboards.
Better task visibility.
More consistent follow-up workflows.
This is where the EMR has to become more than a place to store completed notes.
It has to become a clinical guardrail.
- Why Hospices Need This Now
The 2026 hospice environment requires stronger documentation before the record is signed — not after the risk is discovered.
HOPE is now part of the hospice quality reporting environment, replacing the Hospice Item Set as of October 1, 2025. CMS has also proposed additional hospice transparency measures, including public reporting tools tied to quality reporting compliance, and has discussed hospice spending variation analysis through SSVI in the FY 2027 proposed hospice rule.
Add ADRs, surveys, payment scrutiny, and now the national hospice enrollment moratorium, and the message becomes clear:
Hospice documentation must be more complete, more specific, and more defensible.
Moving From Chart Completion to Documentation Intelligence
The hospices that are best prepared for this environment will be the ones that treat their EMR as more than a digital filing cabinet.
Chart completion is no longer enough.
Hospice teams need documentation intelligence.
They need workflows that help clinicians capture the right information, surface risk before sign-off, support patient-specific care plans, and strengthen the record before it becomes a survey, ADR, or audit issue.
That is exactly why we built Hospice Audit Guard Co-Pilot™ by HospiceWorks.
It helps hospice teams strengthen admission and visit documentation before risk becomes a survey, ADR, or audit problem.
The moratorium is here.
The question is no longer whether the chart was completed.
The question is whether the record is strong enough to defend the care.
Request a 15-Minute Moratorium Risk Audit
About the Author
Ramon Sanchez is the founder of HospiceWorks, a hospice EMR built to help agencies improve clinical workflows, reduce documentation burden, and strengthen compliance readiness. HospiceWorks includes Hospice Audit Guard Co-Pilot™, a proactive documentation defense tool designed to help hospice teams identify documentation risk before sign-off.
Connect with Ramon on [LinkedIn] https://www.linkedin.com/in/ramon-sanchez-009689165/
Sources for Article
CMS, “CMS Announces Aggressive Nationwide Crackdown on Fraud with Six-Month Hospice and Home Health Agency Enrollment Moratoria.”
CMS, “Provider Enrollment Moratoria.”
Federal Register Public Inspection Notice, “Announcement of Nationwide Temporary Moratorium on Enrollment of Hospices.”
CMS, “Hospice Outcomes and Patient Evaluation (HOPE) Technical Information.”
CMS, “CMS Proposes New Transparency Measures to Strengthen Oversight of Hospice Providers.”
Federal Register, “FY 2027 Hospice Wage Index and Payment Rate Update and Hospice Quality Reporting Program Requirements.”